Respiratory viruses cause huge health challenges, especially among those with weak immune systems. Cumulative global incidence of SARS-CoV-2 is estimated to be over 775 million since 2020. Although we thought it would come and go, it didn’t. Many people are reporting persistent symptoms and or feeling poorly after infection and/or receiving the vaccine, including boosters. And influenza is no less concerning at billions of annual cases worldwide, with 3–5 million cases causing severe disease and 290,000–650,000 respiratory fatalities.
Although these viruses primarily affects the respiratory tract, symptoms are known to impact multiple organs and systems, resulting in a range of persistent symptoms not just including respiratory symptoms (such as coughing and difficulty breathing / chest tightness), here’s a longer list:
- cardiovascular symptoms (such as chest pain and palpitations),
- exercise intolerance,
- gastrointestinal symptoms (such as diarrhea and constipation),
- anxiety and sleep disturbances,
- cognitive symptoms (such as memory impairment and difficulty concentrating),
- musculoskeletal symptoms (such as joint and muscle pain),
- dermatological symptoms (such as rashes and alopecia—hair loss),
- fatigue and malaise.
Taken together, these lasting health conditions lead to poor quality of life and physical functioning—a detrimental impact on various aspects of meaningful daily activities, including work, study, and interpersonal relationships.
It remains uncertain how and why these symptoms persist and there are many thoughts in the research community. Certainly, individuals with weakened immune systems are generally more susceptible to severe illness.
Let’s step back and explore how these viruses work to cause illness and become so infectious
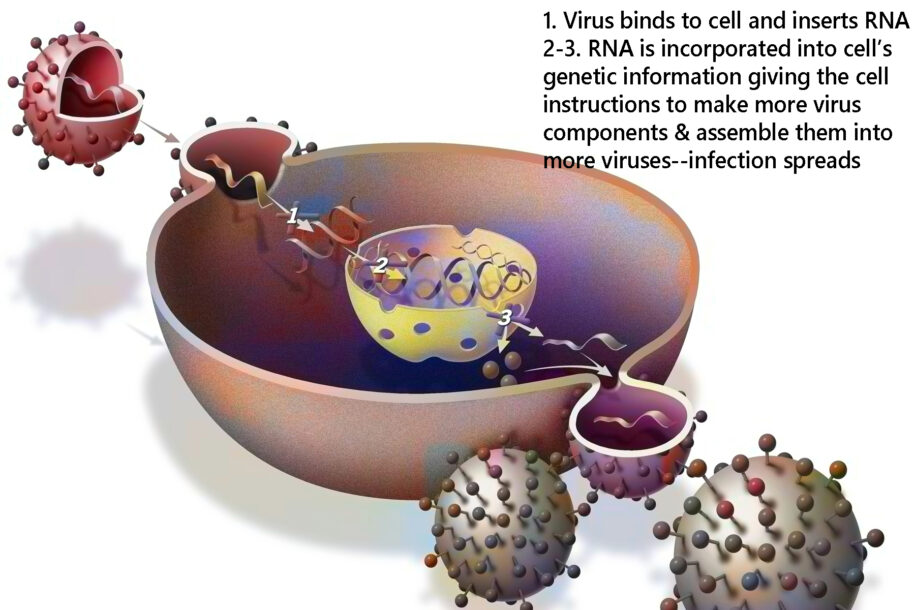
Called “retroviruses” because they use a genetic blueprint called RNA rather than the DNA that normally is a cell’s set of instructions:
- These viruses bind to human (or other animal) cells and insert their RNA into the infected cell’s nucleus and then into it’s DNA blueprint.
- Now, each time the cell tries to follow it’s own genetic instructions, it is commanded by the virus’ genetic info to also make more viral bits.
- Then, these viral components are assembled into complete viruses and shed from that cell to infect more.
The immune system responds to this by attacking the “foreign invaders” including the whole virus, parts of it if a vaccine and/or it’s simple proteins, and/or (if a vaccine response) the various chemicals in the vaccine that are aimed at stabilizing it or making it more effective.
Because any of these causes can lead to residual symptoms; not one clearly stands out. The possibilities include:
- Residual COVID spike protein (that’s the halo, or corona, around the virus that allows it to attach to and infect cells),
- mRNA-infected cells (these program cells to make more viral particles and spike protein),
- Residual vaccine components including mRNA, and lipid nanoparticles (very small fatty particles thought to enhance vaccine activity—these are so small they can get into the cell nucleus),
- Whether an individual experienced SARS-COVID, Flu, or not, post vaccine syndrome (and especially after one or more boosters) can have very similar symptoms. One thing, whether or not receiving the vaccine can cause components to shed to other people is controversial but likely,
- Alterations in immune cell profiles,
- The infection was a trigger for an autoimmune situation (the body can attack itself anywhere),
- Other viruses already in the body, whether dormant or not, are reactivated,
- Other factors such as prions (all cells are programmed to make proteins as building blocks for many things. If these are misfolded, they are called prions and can cause nerve system degeneration, especially the brain). Prions are defective proteins commonly made by yeast forms, viruses, and, importantly, gut microbiome dysbiosis.
But which one is it??? We need to know in order to find the clinically appropriate remedy!
That’s where the new test kits from Ulan Nutrition Systems come in. I have mine, I have the protocols, and best of all: These have been working well to help resolve long viral symptoms for many thousands.
The other clinicians I train with, as well as many clients, report a date coincidence with persistent symptoms and either knowing they had COVID or after receiving the vaccine. Nearly half who have multiple and lasting symptoms look at possible causation even though we can’t specifically assign cause—of course people who don’t have symptoms don’t mention a problem.
This is why, at every Follow-Up or New Client appointment I’ll be checking for this possibility using Nutrition Response Testing and the new Post Pandemic test kit—whether or not you have reason to believe there has been an exposure.
1. Heal the gut
These vriuses alter the gut microbiome– a diverse community of microorganisms (i.e., bacteria, viruses, fungi, archaea) that reside along the gastrointestinal tract and play roles in immunity, defending against pathogens, and supporting nutrient metabolism. Elevated disease-causing bacteria (pathogenic) and decreased beneficial bacteria are involved in diseases of many organs and systems including inflammatory bowel disease (IBD), irritable bowel syndrome (IBS), colorectal cancer, obesity, type 2 diabetes, psychiatric disorders, and neurodegenerative disorders. Additionally, while all of us have yeast populations living in our gut, they need to be in a beneficial form rather than the form that can sneak out of the gut and invade other organs and systems.
There are at-home steps you can and should take to address a gut healing program by encouraging beneficial bacteria. As for buying probiotics, in clinical trials, some worked and some did not.
2. Dissolve the spike protein and prions if a factor
Prions are misfolded proteins created by various immune factors: Virus, bacteria, yeast, parasites… Specific enzymes (but not all) will digest (if you will) these malformed proteins and also the spike proteins of COVID. Both Standard Process and Allegany Nutrition Systems have blends depending on the type of enzyme we need. Again, I primarily use Nutrition Response Testing to determine this.
3. Improve immune status—depending on the cause of your symptoms (viral or other) we can select appropriate remedies
Improve antioxidant status
Interestingly, most of my clients have poor antioxidant levels. These can be seen through basic blood labs especially liver enzymes and Nutrition Response Testing. More detailed tests aren’t necessary if we can see these through the basic tests. While there are several good clinical trials exploring Omega-3 Fatty Acids and/or Coenzyme Q10, these must be taken in the right amounts and often with other things that make them work.
Coenzyme Q10 (CoQ10) supports mitochondrial function, where all cells produce energy. This is often impaired in Long COVID. As a critical element in mitochondrial energy production, CoQ10 helps alleviate symptoms of fatigue and muscle weakness, indirectly aiding cognitive recovery by enhancing physical endurance and reducing oxidative stress.
Whatever you do, please pretty please improve antioxidant status by increasing vegetables and decreasing premade groceries and convenience “foods”/snacks.
Yet, with so many natural approaches, medical guidelines still focus on pharmaceutical approaches:
My comments based on medical literature in italics.
- Vaccines (Why is it that most vaccinated individuals still become infected? Including repeat infections?) The CDC (Center for Disease Control) acknowledges the prevalence of Flu and COVID among fully vaccinated persons yet these are one of the strongest prevention guidelines.
- Antiviral drugs (possibly derived from infected individuals or snake and other animal toxins.) Sadly, most are considered ineffective, or have unwanted side effects, as evidenced by the ever-increasing reports of viral resistance, additional viral infections, and the emergence and re-emergence of viral epidemics in relatively short periods of time, as observed for H1N1, Ebola, and zika virus (ZIKV), and all the CORONA viruses.
- In fact, current guidelines suggest treatment with an antiviral drug starting within 48 hours if exposed and vaccinated, for 5 days, and if unvaccinated guidelines suggest prevention with oseltimivir (Tamiflu) or zanamivir taken continuously through the flu season. (Side effects include gastrointestinal issues such as nausea, vomiting, and diarrhea, and/or breathing issues. Rare but serious side effects can also occur, including severe skin reactions and neuropsychiatric events.
- Antiparasitic or antimalaria drugs (Ivermectin, chloroquine, hydroxychloroquine, quinine, and others) are no longer protected under patent laws as they are older—thus not part of current medical guidelines.
- Also in the guidelines are cautionary statements not to combine any of medications.
That sums it up.
I’m not going to make your decisions for you. Do what seems best and whatever path you choose, know that there is a solution to any problem that may occur. Call me 907-222-1824
References:
Batta, I., Kaur, T., & Agrawal, D. K. (2023). Distinguishing Swine Flu (H1N1) from COVID-19: Clinical, Virological, and Immunological Perspectives. Archives of microbiology & immunology, 7(4), 271–280.
Bhattacharjee, B., Lu, P., Monteiro, V.s. et al. (2025) Immunological and Antigenic Signatures Associated with Chronic Illnesses after COVID-19 Vaccination. British Medical Journal (Yale), Preprint at medRxiv 2025.02.18.25322379
Duraffour, S., Andrei, G., Topalis, D., Krečmerová, M., Crance, J. M., Garin, D., & Snoeck, R. (2012). Mutations conferring resistance to viral DNA polymerase inhibitors in camelpox virus give different drug-susceptibility profiles in vaccinia virus. Journal of virology, 86(13), 7310–7325.
Lau, R. I., Su, Q., & Ng, S. C. (2025). Long COVID and gut microbiome: insights into pathogenesis and therapeutics. Gut microbes, 17(1), 2457495.
Livieratos, A., Gogos, C., & Akinosoglou, K. (2024). Beyond Antivirals: Alternative Therapies for Long COVID. Viruses, 16(11), 1795.
Luong, Q. X. T., Hoang, P. T., Ho, P. T., Ayun, R. Q., Lee, T. K., & Lee, S. (2025). Potential Broad-Spectrum Antiviral Agents: A Key Arsenal Against Newly Emerging and Reemerging Respiratory RNA Viruses. International journal of molecular sciences, 26(4), 1481.
Stefano, G. B., Büttiker, P., Weissenberger, S., Anders, M., Raboch, J., Ptacek, R., & Kream, R. M. (2023). Potential Prion Involvement in Long COVID-19 Neuropathology, Including Behavior. Cellular and molecular neurobiology, 43(6), 2621–2626.
Vilas Boas, L. C. P., Campos, M. L., Berlanda, R. L. A., de Carvalho Neves, N., & Franco, O. L. (2019). Antiviral peptides as promising therapeutic drugs. Cellular and molecular life sciences : CMLS, 76(18), 3525–3542.
Leave a Reply
You must be logged in to post a comment.